Allgemeines
PIN
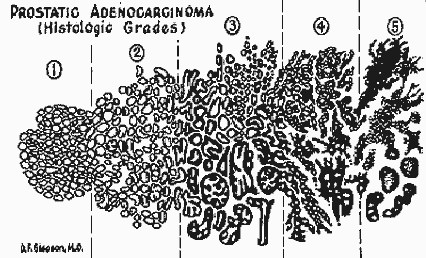
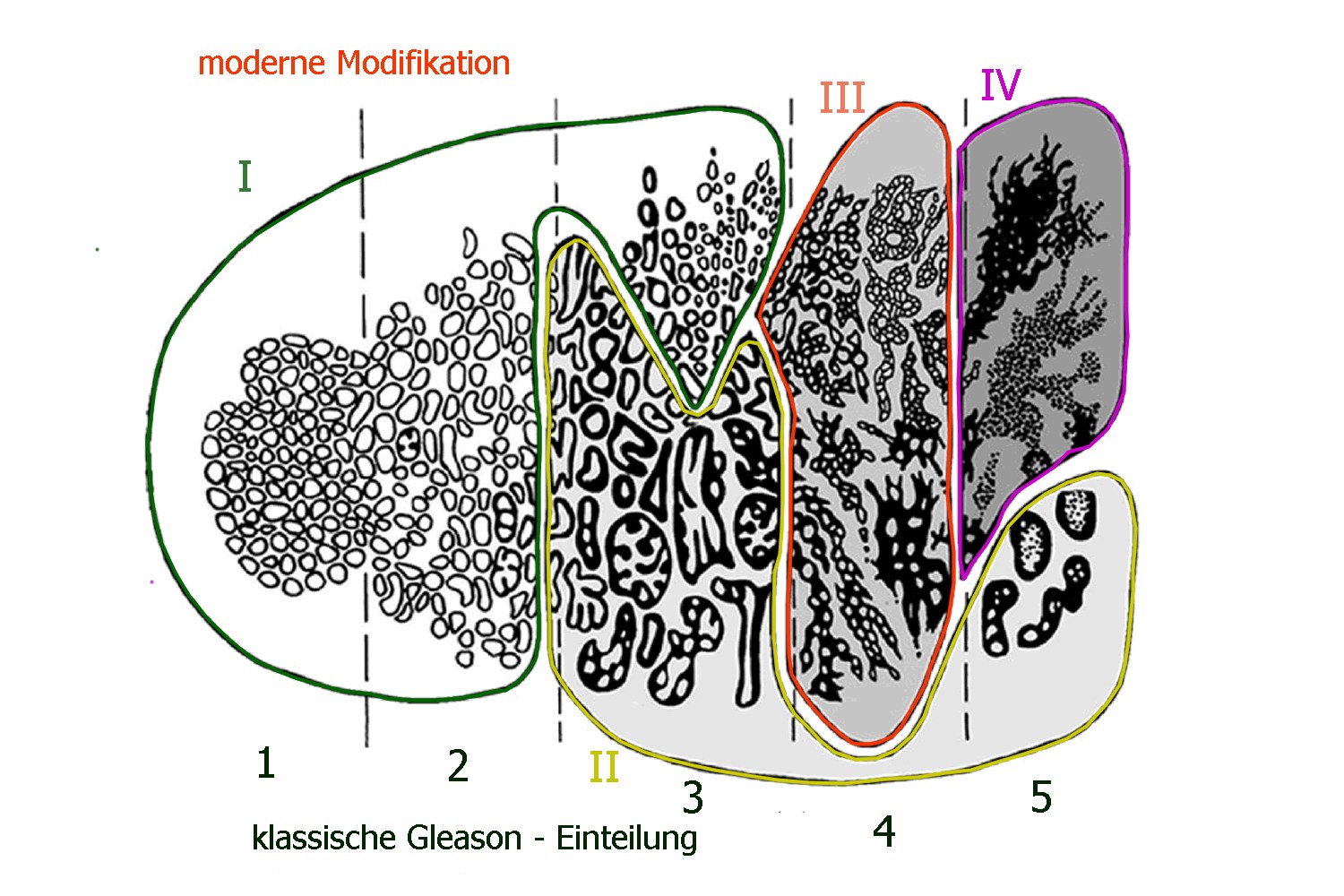
Gleason - Score
| Histologisches Grading an Hand von Stanzbiopsien oder OP-Präparat. | ||
| Gleason - Pattern | Wachstumsmuster: 1 = hoch differenziert, 5 = maximal entartet | |
| Auswertung | Die 2 häufigsten Stufen werden addiert. | |
| Skala | Der niedrigste Wert ist 1+1 = 2, der höchste 5 + 5 = 10 | |
Prognose-Gruppen
Histochemie
ERG
Molekularbiologie
| Gen | % Mutation | Mechanismus | Art der Mutation | |
| AR Gen | 62,7% | Androgen - Signaling | Amplification, splice variants, Mutation | |
| TP53 | 53,3% | Zellzyklus oder Tumorsuppressor | Mutation, copy loss | |
| PTEN | 40,7 % | PI3K–AKT - Regulator | Copy loss, Mutation | Bei Funktionsverlust hohes Risiko einer Hormonresistenz |
| ETS | 56,7 % | Transkriptions - Regulator | Gen fusions | |
| BRCA2 | 13,3 % | DNA - Repair | Copy loss, Mutation | |
| KMT2C | 12,7 % | Chromatin modifier | Mutation | |
| FOXA1 | 12,0 % | Androgenrezeptor assoziiert | Mutation | |
| ZBTB16 | 10,0 % | Androgenrezeptor assoziiert | Copy loss | |
| RB1 | 9,3 % | Zellzyklus | Copy loss | |
| APC | 8,7 % | Wnt - Pathway | Copy loss, Mutation | |
| CHD1 | 8,0 % | Chromatin - Modifier | Copy loss, Mutation | |
| SPOP | 8,0 % | Androgen - Signaling | Mutation | |
| ATM | 7,3 % | DNA - Repair | Copy loss, Mutation |
AR = Androgen-Rezeptor, nach Daten von (4)
Gleason 3 + 3
SCPCa
DD Urothelkarzinom
ISUP
Teil von
Quellen
Prediction of prognosis for prostatic adenocarcinoma by combined histological grading and clinical staging.
J Urol 111 (1974):58-64.
2.) Epstein JI1, Egevad L, Humphrey PA, Montironi R; Members of the ISUP Immunohistochemistry in Diagnostic Urologic Pathology Group:
Best practices recommendations in the application of immunohistochemistry in the prostate: report from the International Society of Urologic Pathology consensus conference.
Am J Surg Pathol 38(2014):e6-e19. doi: 10.1097/PAS.0238.
3.) Dong F, et al.:
Impact on the clinical outcome of prostate cancer by the 2005 international society of urological pathology modified Gleason grading system.
Am J Surg Pathol 36(2012):838-43. doi: 10.1097/PAS.0b013e3182486faf.
4.) Robinson D, Van Allen EM, Wu YM, et al.:
Integrative clinical genomics of advanced prostate cancer.
Cell 2015; 161: 1215-28
