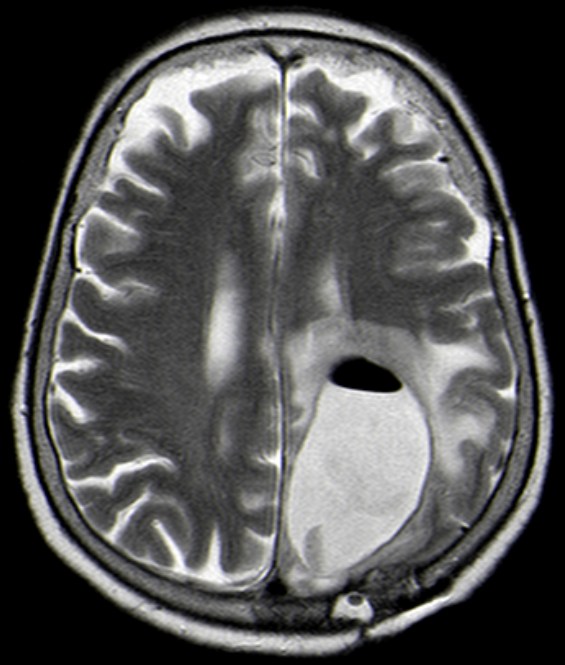
Therapie des Glioblastoms
Allgemeines
Operation
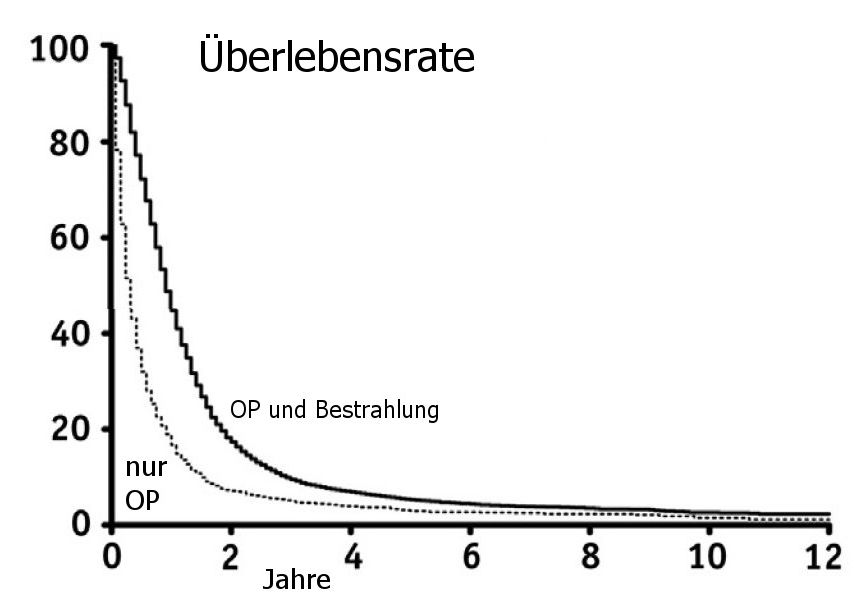
Modifiziert nach (4). SEER-analyse.
Chemotherapie
Radiochemotherapie
| Studie | Arm | OS | PFS | Patienten | Bemerkungen |
| ANOCEF (8) | BSC | 3.9 | 1.2 | 42 | Referenzgruppe HR 1.00 |
| 50 Gy / 1,8Gy ED | 6.7 | 3.4 | 39 | RT besser HR (OS): 0.47 (0.29–0.76) | |
| NOA-08 (9( | 60 Gy / 2Gy ED | 9.6 | 4.7 | 178 | kein Unterschied |
| Temozolomid Dose-dense | 8.6 | 3.3 | 195 | NOA-8 enthält 11% anaplastische Astrocytome | |
| Nordic Clinical Brain Tumour Study Group (10) |
60 Gy / 2Gy ED | 6.0 | NR | 100 | Referenzgruppe HR 1.00 |
| 34 Gy / 3,4Gy ED | 7.5 | NR | 98 | HR (OS): 0.85 (0.64–1.12) | |
| Temozolomid | 8.3 | NR | 93 | HR (OS): 0.70 (0.52–0.93) | |
| CCTG/EORTC/TROG (6) | 40 Gy / 2,66 Gy ED | 7.6 | 3.9 | 281 | Referenzgruppe HR 1.00 |
| 40 Gy / 2,66 Gy ED + Temozolomid, dann Temozolomid |
9.3 | 5.3 | 281 | HR (OS): 0.67 (0.56–0.80) |
Nach diesen Daten Sollten Patienten über 60 Jahre mit RT und Temozolomid behandelt werden, wenn der AZ das zulässt.
Target - Therapie
Optune
Quellen
Intensive chemotherapy improves survival in pediatric high-grade glioma after gross total resection: results of the HIT-GBM-C protocol.
Cancer 2009; 2: 2
2.) Hegi ME, et al.:
MGMT gene silencing and benefit from temozolomide in glioblastoma.
NEJM 352(2005):997–1003
3.) Stockhammer F, et al.:
Continuous low-dose temozolomid and celecoxib in recurrent glioblastoma.
J Neuro-Oncology 2010;100:407-15
4.) Rusthoven CG, et al.:
The Impact of Adjuvant Radiation Therapy for High-Grade Gliomas by Histology in the United States Population.
Int J Radiation Oncol Biol Phys 2014;90:894-902. http://dx.doi.org/10.1016/j.ijrobp.2014.07.046
5.) Marko NF, et al.:
Extent of Resection of Glioblastoma Revisited: Personalized Survival Modeling Facilitates More Accurate Survival Prediction and Supports a Maximum-Safe-Resection Approach to Surgery.
J Clin Oncol 2014;32:774-782. DOI: 10.1200/JCO.2013.51.8886
6.) Perry JR, Laperriere N, O’Callaghan CJ, et al.:
Short-course radiation plus temozolomide in elderly patients with glioblastoma.
N Engl J Med 2017; 376: 1027-37.
7.) Rusthoven CG, Koshy M, Sher DJ, et al.:
Combined-modality therapy with radiation and chemotherapy for elderly patients with glioblastoma in the temozolomide era: a National Cancer Database analysis.
JAMA Neurol 2016; 73: 821-8.
8.) Keime-Guibert F, Chinot O, Taillandier L, et al.:
Radiotherapy for glioblastoma in the elderly.
N Engl J Med 2007; 356: 1527-35.
9.) Wick W, Platten M, Meisner C, et al.:
Temozolomide chemotherapy alone versus radiotherapy alone for malignant astrocytoma in the elderly: the NOA-08 randomised, phase 3 trial.
Lancet Oncol 2012; 13: 707-15.
10.) Malmström A, Grønberg BH, Marosi C, et al.:
Temozolomide versus standard 6-week radiotherapy versus hypofractionated radiotherapy in patients older than 60 years with glioblastoma: the Nordic randomised, phase 3 trial.
Lancet Oncol 2012; 13: 916-26.
11.) Laperriere N, Zuraw L, Cairncross G, Cancer Care Ontario:
Practice Guidelines Initiative Neuro-Oncology Disease Site Group.
Radiotherapy for newly diagnosed malignant gliomain adults: a systematic review.
Radiother Oncol 2002;64:259–73.
12.) Mason WP, et al. for the Canadian GBM Recommendations Committee:
Canadian recommendations for the treatment of glioblastoma multiforme.
Curr Oncol 2007;14:110–117
Teil von
